
I started nexium tonight. 3 caps 1x a day. Did 14 days of UG, then a week of sand clear but my guy is getting grumpy again, not eating well again, and standing funny again (like an elephant on a ball). We’ve been battling his health issues for a couple years now. I do believe now that he has ulcers. He was remarkably better while on UG and his funny stance went away! For a couple years now we thought that stance was due to hind end joint issues, but after seeing the difference I believe it’s from ulcer pain. I will report back in a week and let you all know how it’s going! Thank you so much for this info! A friend told me about it!
6 Likes
I have a horse just down to his last 5 doses of GG. We begin to start tapering off. Does he still need to fast before and for an hour past feeding the GG?
1 Like
This thread is specific to Nexium. You may want to start a new thread about your Gastrogard question.
4 Likes
No need or benefit to tapering, there’s no dimmer switch in horses, per Dr Ben Sykes. And the rebound is not only short-lived, like 2-3 days, it doesn’t even start until the drug is stopped.
1 Like
What Sykes actually says about tapering is this:
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10093336/
“Collectively, the findings of the recent work suggest that a brief period of RGH [rebound gastric hyperacidity] might occur within a 48–hour window following the administration of the last dose of omeprazole, but that the effect is not prolonged. As such, the authors currently do not recommend tapering of omeprazole for treatment durations of ≤8-weeks. Instead, the authors focus on the 24–48-h period following the administration of the last dose of omeprazole, making sure that horses are provided with appropriate roughage during this time, and that they are not exercised nor transported during the expected, albeit brief, RGH event that might occur in this window. Further studies are needed to evaluate the impact of longer duration treatment on serum gastrin and CgA concentrations with tapering recommendations adjusted accordingly.”
So while he does not recommend a taper based on this single research study comprising a handful of horses, he does have recommendations for the period after discontinuation, and states that further study is necessary to determine if this applies to extended treatment durations.
To sum up the two papers published about this study: (the first is published here.) The cohort was a small group (14 horses) and a very homologous population; all geldings, all housed the same, all fed the same, and all trained the same. While that helps with keeping outside factors from muddying the data, it DOES make it more difficult to apply these results to different populations.
Stomach acid level was monitored not directly in the stomach but by blood level. In humans, we can monitor stomach acid levels via serum gastrin and serum CgA, so Sykes also used those markers here. Gastrin levels rose (inversely correlated to stomach acid level) at the beginning of treatment, stayed high through treatment, then fell below baseline upon discontinuation of omeprazole. Gastrin returned to baseline within 2-4 days. CgA did not rise, so that doesn’t seem to be a marker we can use in horses, unlike in people. Validating how serum gastrin relates to stomach acid in the equine wasn’t done here in this paper, perhaps it was done elsewhere. I did not see an obvious cite regarding that.
Sykes also says in this paper:
A rapid reccurrence of ESGD in 83% of horses within 3 days of omeprazole withdrawal has been reported [by Sykes, in the paper discussed below]. In humans, the occurrence of rebound symptoms and reccurrence of gastric disease have been observed after omeprazole withdrawal, considered to be the result of hypergastrinemia and RGH. Increased serum gastrin concentration in response to omeprazole treatment observed in our study might contribute to the short‐term development of RGH and help explain the rapid reccurrence of ESGD. However, further investigation of serum gastrin concentrations each day after omeprazole withdrawal using concurrent gastroscopy is required to determine this outcome.
Sykes states that the gastroscopy portion of this study is published here.
This paper describes treating horses (the same population as above) with omeprazole for 28 days, then 3 days unmedicated, then treatment resumed for another 28 days, then another 1 day withhold. Horses were scoped at day 0, 28, 31, 59, 62.
They also tried a similar set up with 21 days treated, two days withhold but with a OTC buffer, followed by one day with nothing.
Withholding for 3 days saw an increase in ulcers across the board. Pictures say it best:
Squamous (“normal” ulcers):
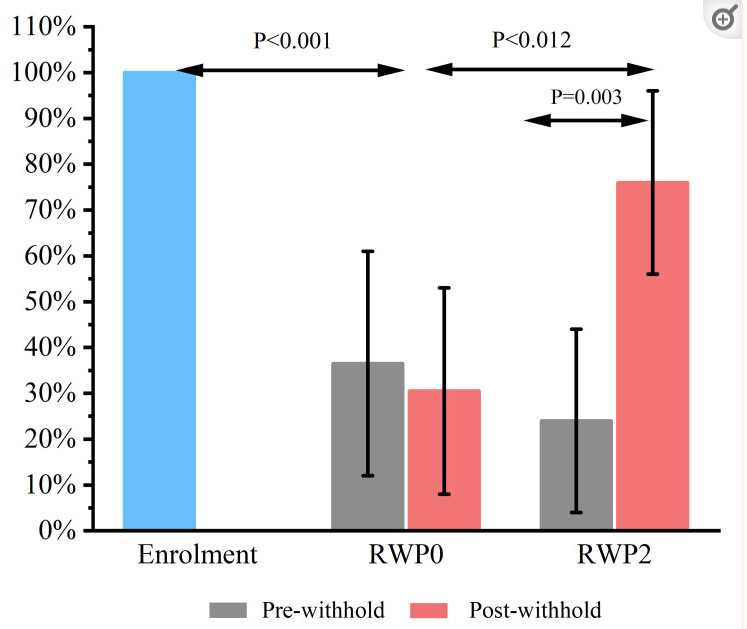
Everyone had ulcers on day 0. 40ish% had ulcers pre one day withhold, slightly lower post one day withhold. 25% had ulcers pre 3 day withhold, 75% post 3 day withhold.
Glandular ulcers:
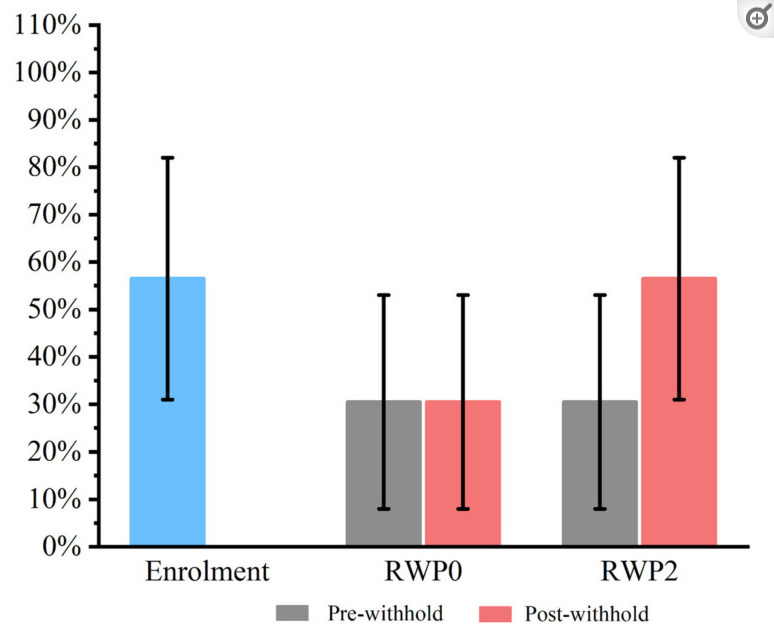
About 55% had glandular ulcers at day 0. 30% pre and post 1 day withhold. 30% pre 3 day withhold, 55% post three day withhold.
It’s apparent that it takes very little time to redevelop ulcers following treatment–as little as three days. This is also the window of “rebound” per the serum gastrin data Sykes published, which is presumably driving his recommendation for no hauling, no riding, and “appropriate roughage.”
None of these papers discuss what happens with tapering, and Sykes does not cite any data regarding that. If he’s researched that, he is not referencing that work here, even as “unpublished data.”
@JB you’ve stated repeatedly that Sykes has done that research and that “rebound doesn’t start until the drug is stopped.” Do you have a paper in which that work has been published and undergone peer review? I haven’t seen that published.
Regardless, even if that’s true, the tapering/not tapering question is a lot more complex than “Sykes says you don’t need to taper” and it’s–at best–grossly over simplifying to boil down an entire avenue of very nascent research to a single sentence.
8 Likes
I couldn’t figure it out, was there any benefit from OTC buffer during the rebound period?
Hmmmm, some? We went from 20-45% with a 3 day hold with an OTC buffer, compared to 25-75% without.
It can’t hurt, and might help 
Sykes sums of his caveats about it here:
The use of a commercial nutraceutical supplement during the RWP appeared to reduce the rate of recurrence of ESGD in the present study. This is consistent with a previous study that evaluated the effect of a near-identical formulation over a 28-day period following the discontinuation of omeprazole treatment, in which protective effects for both ESGD and EGGD were demonstrated [17]. However, an important limitation of the present study was that no control group was used in Part 2 of the study, with the results from Part 1 being used as the control instead. Although the horses were otherwise managed under identical conditions, the different durations of treatment (21 days in Part 2 vs. 28 days in Part 1) might have influenced the likelihood of RGH as a contributory factor. The authors consider this unlikely as the magnitude of hypergastrinemia, the main driver for RGH does not differ between 3 and 4 weeks of omeprazole treatment (unpublished data). Given these limitations, further study using an appropriate control group is required before firm conclusions can be drawn. Other nutraceuticals have been demonstrated to have protective effects against ESGD under similar conditions [33]. As such, the strategic use of specific nutraceuticals during RWPs or following the discontinuation of omeprazole might be useful in reducing the risk of recurrence of ESGD.
The supplement this study used was GastroAid Recovery, and it was dosed twice daily.
It’s in his video which I’ve posted several times
As I said, I am asking specifically about peer reviewed literature. Where is it published?
1 Like
You’ll just have to email him and ask. I don’t keep up on his daily work or ask what state his research is in.
2 Likes
Ha! What? You can’t substantiate your claims, so you’re telling me to?
I know you think I’m an asshole for asking for data, @JB, but saying “Sykes says you don’t have to taper” is really missing a whole lot of his recommendation–which is even discussed in the video you linked!–and ignoring a massive recurrence rate. Sykes simply doesn’t just say you don’t need to taper–he has several other recommendations on how to support the horse once discontinuing the PPI. And there are so many unanswered questions–what’s the recurrence rate with no taper and the support he recommends? What’s actually going on in the stomach vs the serum gastrin? Are there other mechanisms that could contribute to rebound gastric hyperacidity in equines or ulcer recurrence that we don’t see in humans?
Let’s talk about what he does say in the 15 minute video published to the very well respected journal of…Facebook.
This begins about 7 minutes in, this is where he discusses tapering the omeprazole dose.
Here’s the image he shows. I recognize this from one of his papers investigating dose, but haven’t yet pinned it down to exact paper. He says it’s from his PhD.
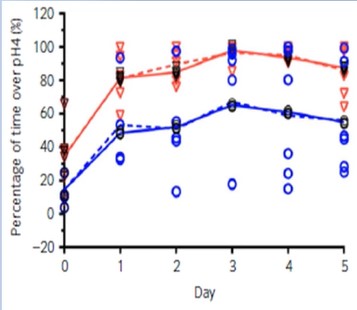
From the video:
But, @JB, he never actually tapered these horses. He NEVER started at 4 mg per kg and maintained that and reduced the dose to see what happened. He never compared a taper to no taper in outcomes. He never investigated differing tapering regimens. He looked at two different doses individually. Yes, there is a dose dependent variable. Yes, horses respond to omeprazole in different ways.
But we still don’t know how horses (in general) or horses (specifically as individuals) respond to a taper. This data of “horses respond differently” seems to at least suggest that YES, absolutely, there are indeed some horses out there that might benefit from a taper. Some horses may not. There’s probably no way to know which you’ve got without stuff that most owners aren’t interested in. At the least, there is likely little harm in tapering, and some potential for benefit. The gastrin data seem to suggest a taper does not need to be terribly extended. (I’d also like to point out that Sykes is NOT including this “there’s no dimmer switch” concept in this sort of paper.)
A recurrence rate of 83% is jaw dropping. Treating for 4 weeks and sudden discontinuation with no post med support = more than 4 out of 5 horses popping ulcers in THREE DAYS. When you say “Sykes says you don’t need to taper,” that’s what you’re telling people to do. If you’re going to continue to summarize this all down into one bullet point, at least include what else he says about post treatment support.
This is hardly settled science, and there’s so much work yet to be done.
11 Likes
I just heard about using nexium for ulcers in horses. I have read through a lot of the posts here and have a couple things to think about
The capsule holding the drug is not the enteric coating. The coating is on the little pills inside. The capsule is a gel which is just used as a delivery method
And also, if it needs to get to the hindgut unaffected, how does Ulcergard or Gastrogard paste accomplish this.
If the horse has an ulcer, not scoped, will the dose recommended here heal the ulcer?
Because those pastes are buffered so the omeprazole itself survives the stomach.
Scoping doesn’t make or break healing, what does is whether you’re using the appropriate drug for the type of ulcer. (Es)omeprazole works best for squamous, but not glandular or pyloric.
I’m not sure which dose you’re referring to, but if you’re talking about the 40-80mg (2-4 otc esomeprazole capsules) then lots of horses have scopes showing that dose did, and did not work. Some needed a much higher dose, like 12-14 capsules (for an average 1000-1200lb-ish horse). Sometimes 60 days is needed, not just 30. So there’s no guarantees with esomeprazole, or even omeprazole.
3 Likes
Thank you!
Continuing with this long thread…
I have read all 945 on here and feel (relatively) ready to give this a go. First a few clarifications:
-
The first study was the least amount and that is where the 40mg comes from. Then an extra 20 in case one doesn’t get through (bitten).
-
We want to do the smallest dose of Nexium possible, mainly because these meds can cause issues with the hind gut including hind gut ulcers.
-
We know the pH is above 4 at 6 hours at this dose but we don’t know what it is at 12 hours?
-
Some say don’t add a buffering supplement (like Purina’s) with it bc too much buffering but some say to do so if you are concerned about the Nexium being absorbed? Clarification anyone?
-
Results vary. Research is showing more and more that different horses absorb at different rates.
-
If my pony gets worse, he probably has hind gut ulcers not stomach ulcers.
-
Some people do both Nexium and a hind gut treatment at the same time. Why?
-
Generic seems to work as well as brand name.
-
I think that’s everything but I’ll add later if something comes up.
My new pony… I’m not convinced he has ulcers but I do think he has something going on with him.
He’s a cribber and very nervous. Just “not right” but I don’t know what “right” looks like for him.
Eats pretty well, no diarrhea. Suggested to me he may have ulcers so I am going to give the Nexium a try, with a blessing from my vet who is hugely curious regarding how this is going to work out.
I am guessing he weighs 800-900#. Deciding whether to try 40 2x a day or 60 once a day. I’ve already ordered them. Thanks Xanthoria for the link!
I look forward to you all’s responses. Lydia
5 Likes

Very cute guy! What a nice picture!
Something else that does seem to be shown in the literature is that dosing as close to an empty stomach as you can is beneficial. That doesn’t mean you’ve got to fast your horse, but dosing when they’re less likely to have a stomach full of hay is more likely to have a positive result than if you dose after they’ve had their fill.
I manage this easily by dosing with dinner. My horses mill around the gate in the evenings rather than graze. By the time they come in, they haven’t eaten in awhile.
Best of luck, hope it helps!
5 Likes
I assume you put it in their dinner?
Thanks for this wonderful thread.
Personally, since we don’t have good data on longer term effect (aka past 6 hours), I’d do twice a day if possible. But as this thread has shown, we are extrapolating from minimal research and everyone is doing that slightly differently. Do what seems best to you!
Anecdotally, I had the outward signs of success treating 2x a day with a higher dose (12 pills), and outward signs of failure treating 2x a day with a lower one (6, and 3 pills). Now, since I didn’t scope, who knows what other factors were at play. However, a round of Abler pop rocks gave me a better result following the lower dose failure, so  . This was all on the same horse, FWIW.
. This was all on the same horse, FWIW.
3 Likes