Nurses will instruct you on how to get out of bed and get to the bathroom - the very first day ! They will have you Up and walking the halls with a walker the day after surgery ~ they will guide you all the way ~ I promise !
OT will visit your home before the surgery to help make modifications - example = our couch was too low ( according to protocol - bending at hip) H had to have the couch raised / think 2x4’s nailed to the bottom of the couch,to enable me to sit in the living room. You will be advised on purchasing a raised toilet seat / fits over your toilet and a tub bench seat / enables you to sit and bring your legs over the tub - then you sit using the hand held spray ~
There is usually a meeting with others headed to “replacement part” surgery - required / they will review everything !
It’s overwhelming and it’s easy to suffer from ‘analysis paralysis’ reading and asking?s BUT ~ you are not responsible for performing the surgery or prepping - your team will guide you / support you : make sure it’s all safe ~ but it’s a process and you don’t want to rush it / there will be BORING DAYS • but you’ll get there !
You’ll be back in the saddle in 60 days ~ You’ll GET YOUR LIFE BACK !
lastly during the wee hours of the morning when you can’t sleep - please know there are videos showing how to use the bathroom aids ~ all models are clothed !
Thanks, @Zu_Zu - as always, you are very kind and supportive!
This is all such useful information – I had no idea that I would get so much help! I hope that’s not just local to you guys and not to Northern Virginia, but I will certainly ask the orthopedist this Friday at the consult.
My DH has had both hips replaced. The second one must be 14 years old now. He was out of pain pretty much immediately after the surgery. It was quite miraculous, really.
They didn’t let him out of the hospital until he could navigate stairs, etc., which I think was three nights the first time round and two nights the second.
The thing that made the biggest difference in his recovery time between the first and second surgeries was the anesthesia. First time round it was the full intubation knock-out, second time around he went for the epidural and twilight sedation. The second was by far the preferable approach as he didn’t have that awful two-week hangover after.
He was released with crutches, never had a walker. We did have the raised toilet seat and the claw for picking things up off the floor and putting on socks. Every home should have one
He was skiing again 12 weeks after his second one. And he would have been 68 and not in great shape when he had it done.
Oh, and all I did was roll up the throw rugs and put them out of the way for a few weeks. No furniture relocation or anything.
Hi Dr_Doolittle,
I’ve just been going thru the process of choosing a surgeon for THR. It’s a pretty amazing surgery. Recent surgery techniques, for the U.S. anyway, have changed a lot in the last few years. Many patients go home same day now, with the anterior and lateral approaches esp.
I expected that the anterior approach was a ‘no brainer’ for me but found it typically uses pretty significant traction to the leg. That’s not a prob for most people but if you have any pre-existing knee probs, be sure to discuss this with your ortho and surgeon. The surgery will have the leg dropped down and away from your body, with the foot rotated outward, traction of about 50#. There’s a special surgical table that allow the leg to be positioned this way. I opted for a lateral approach that doesn’t include traction cuz of quirky knees.
Talk to each surgeon about temp and permanent restrictions. I was surprised that, even among surgeons using the same approach, they may have very different restrictions and for diff lengths of time. Some want you to use antibiotics, permanently, bef a whole list of procedures (dental, colonoscopy). Others dont. Some has positional restrictions, others have literally none. Also make sure to explain current med issues and medication, particularly osteopenia/osteoporosis. Some THR methods have a slightly higher rate of bone fracture during the surgery esp if bone quality is less. Finally, ask whether the surgery will detach/split ligaments on the outside of hip that handle abduction. As a rider, I decided I wanted to avoid that, if poss, since it’s a frequent movement for mounting, lifting legs for changes, etc.
You just do what you gotta do. Having the pain gone and your life back is worth the short-term inconveniences. Your students will understand! Honestly, depending on how you recover, you might be able to return to giving lessons in a few weeks, so long as you stay on the ground and just supervise/observe. You could alternate between sitting and standing as you need. There are accommodations you can make to get back at it sooner!
A lot of your questions (stairs, low chairs, getting up and down, hospital stay or outpatient, showering, etc etc etc) are covered in depth in your pre-op appointments, and you’ll have a lot of them and the information will be gone over multiple times. At least, that what my experience. I had an entire booklet, and several people went through key items with me at several appointments. Making sure your home environment is ready to go, having a good understanding of your restrictions based on the surgeon’s approach, etc etc.
I also joined a social media group as there was one specific to horse riders. That’s been a good one. Everyone’s experiences are different.
The only other thing I forgot to add in my other post is that I mostly slept in the recliner for the first 4 or 5 weeks. Which sucked for me because I am a side sleeper. I hated sleeping in the recliner but I did wake up a lot at night and almost had what I call a restless leg syndrome, where I just need to get up and walk a little bit, and then go back to bed. (AKA the recliner) I could get into bed just fine, but it was a production to get myself propped with a pillow like I need to to get on my side, and then bother my husband in the process. So it was just easier to sleep in the recliner in the living room, so that’s what I did.
Also, for the pooping topic above (because it’s a very real problem when on opiods!!!) but my pre-op staff were very good about educating me about this and told me to buy certain things and just take them. Because right, you’re pretty darn miserable pretty fast if you cannot “go”!
Now I haven’t been through breast surgery, but I did have a friend who had breast enlargement and she was VERY much in pain too for quite a while. From the people I have talked to, those surgeries are more painful than a hip replacement. But of course, everyone is different.
I was utterly shocked that my hip didn’t hurt. Even right after I woke up!! Like honestly, the doctor just sawed off my bone, core-drilled a hole down into it, and it doesn’t hurt. WTH. And I had instant relief from the horrible pain and tightness down the front of my leg - gone immediately. Which was cool. The only thing that hurt was just the muscles and the incision that had to heal. Which I am impressed. My incision is like 3 1/2 inches. That’s it. I have no idea how he got in there with such a small incision!
Someone talked about knee pain above. You’re going to have SOME knee pain after surgery no matter what. And it makes sense. The tendons / ligaments are going to be working differently after surgery and everything is connected. The side of my knee was the most sore I think about 1 week-ish after the surgery. Which got better and subsided. But I had been limping for so long, and “walking wrong” for so long, it’s going to be sore when you start walking correctly again. So expect that.
Yes, I was told the anterior approach puts a ton of stress on your femur due to the angle they have to dislocate you, and there is risk of fracture because of it, and likely worse knee pain after. My surgeon also told me there is a high percentage that have permanent numbness after the anterior approach because you have a nerve that might be in the way when they go in there. So those were some of the reasons why I chose the posterior approach. However, my husband has a friend that did the anterior with another surgery and he’s fine and did great. So you have to decide which surgeon you are most comfortable with.
Thanks so much, I am very grateful for you taking the time to explain everything so thoroughly! I’ll have a list of questions at the consultation, there is so much to ask (and prepare for), but the contributions of posters in this thread have really helped guide me in the right direction.
Might you have a link to the Facebook group you mentioned?
You have received some really good information here. Both my parents had total hip replacement 14ish years ago and I was my mother’s primary caregiver for 2 weeks. My Dad’s procedure went very well. He has always been active. He stayed one night in the hospital and went home relatively pain free. Excellent outcome. My Mother’s procedure was very different. She had a backwards coccyx, had two discs removed and quite a bit of arthritis. She also had low bone density which for some reason was unknown until her surgeon got her on the table. She was in the hospital for 3 weeks and her recovery was very slow. Make sure your surgeon checks your bone density ahead of time. She did get pain relief after and never regretted the choice to have it replaced.
I don’t think there is ever a good time as far as scheduling when to do a surgery that will interrupt everyone’s life( around you) , so it is best to bite the bullet and do it now before the real good outside activity weather gets here?
I don’t have personal experience, just going off my mom and her hip replacement. She was 77 when she had hers. She was determined to be back to normal asap and she was. At 89 now, she still walks daily and does all her activities.
You may miss some riding time but won’t it be nice to ride comfortably when you can ride again??
Good idea to check bone density; I do have osteopenia in one of my hips, I thought it was the left, but it might be the right? I do have an order for another bone density test (last one was about two or or three years ago.) I also have knee arthritis – a ganglion cyst in my right knee, and my left knee has floating cartilage. They both been injected but not recently – the right one is unstable and clicks a lot, but I will be sure to mention that to him, and probably need an updated x-ray of that one as well!
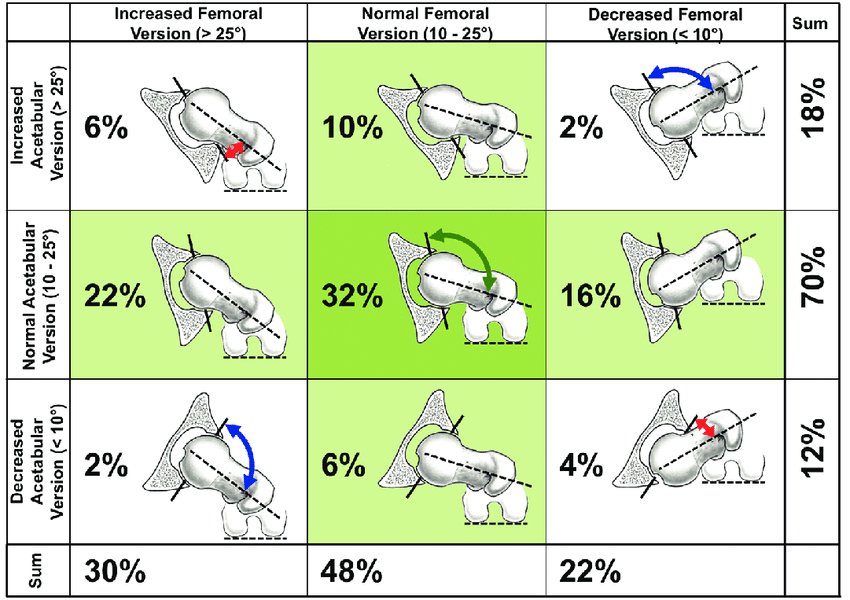
Knee stuff plus hip stuff can be indicative of version abnormality or even something called miserable malalignment syndrome, which is stacking version issues in multiple joints in the leg.
Just one more thing to ask about, because how they orient your new hip does have knock on effects into the knee, so it’s important to know if there’s anything NQR in how those things line up with each other.
3D CT is how version is evaluated. Hip version requires scanning the hip & knee. Knee version might take scanning the ankles? Version is how the angles of the joint relate to each other. Here’s a pic on how acetabular & femoral version interact with each other, and how it relates to the proximal femoral condyle.
A CT is usually part of pre op planning for hip replacement, so sure. Doubt insurance would flinch at all when a hip guy orders a hip CT. I’ve had…geez, several over the years, with no insurance issues.
But yeah, CT is usually how they determine which implant, which size, and how it should be positioned. They don’t (or shouldn’t!!) just go in and wing it
If you can find the space, picking up a massage table–basic ones on Amazon or used ones on FB marketplace can both be found pretty inexpensively–is just fab for rehab. Doing lying down PT on the ground or in bed sux. Sooooo much easier on a table!
Interesting! Finding the room, though - yeah, that’s going to be tough.
Sleeping in a recliner; that would be a good idea (I sit in one in the living room), but trying to sleep in it may KILL my low back. My QLs are very tight and I have to use lumbar support, heat, TENS unit, regular bodywork, trigger point injections, stretching, inversion table etc. to keep them from seizing up. DH said he can bring our daughter’s single bed downstairs and see if he can “make it fit” in the living room. (This should be an interesting experiment! Ha! Yoiks.)

 or prepping - your team will guide you / support you : make sure it’s all safe ~ but it’s a process and you don’t want to rush it / there will be BORING DAYS • but you’ll get there !
or prepping - your team will guide you / support you : make sure it’s all safe ~ but it’s a process and you don’t want to rush it / there will be BORING DAYS • but you’ll get there !




 That’s been a good one. Everyone’s experiences are different.
That’s been a good one. Everyone’s experiences are different.
 over the years, with no insurance issues.
over the years, with no insurance issues.

