
This is sleep deprivation (my horse does the exact same thing and will sometimes fall down). He is not getting enough recumbent sleep, which can be caused by many issues. The first thing to investigate is if he’s not laying down to sleep due to pain. After that is ruled out, it can be caused by insecurity within the herd, issues with the size of the stall, bedding, etc. I’ve not been able to solve it with my horse because I’m limited due to my boarding situation as to what stall I can use and what herd he goes out with.
1 Like
Question for those of you with CA experience: if a horse has lameness caused by CA or another neck issue, will diagnostic blocking of the legs resolve the lameness? IOW, if your horse’s right front lameness resolves with an abaxial nerve block, does that rule out the lameness originating in the neck?
OP, I’m sorry to hear about your horse. So awful how they can be great one day and a medical mystery the next. I hope you can sort it out!
1 Like
I had to go look–mine did block when the issue was the spine. Looked like hocks, blocked to the hocks. Injecting them didn’t help. Then we found the spine stuff.
Here is the thread I started at that time.
i think if budget is a concern, i’d spring for neck rads first (before committing to any other therapy, i mean) to see what we are dealing with - god knows with horse luck you might be barking up the wrong tree. i have heard mixed reviews on PEMF for horses with spinal issues. it seems to work better for other compensatory issues. it is also not cheap.
neck rads were about ~$200. including tranq. by far not the most expensive area i’ve had go under film.
what tack are you selling? if he is your event horse i wouldn’t throw in the towel yet on his stuff… unless you were already considering retiring him.
good luck and keep us updated please.
3 Likes
Interesting! I am going to do chiro but vet recommended waiting at least 30 days.
Yes you’re right. X rays will be the first thing we do… general consensus does seem that the neck could be the culprit.
I am selling hisjump saddle and bridles. His jump saddle was a cheap good deal I just bought a few months ago because his no longer fit, this was a decent fit but not perfect. I just had professionally fitted, so if he is rideable again someday, I will be using my fitter to help me find the perfect fit lol. He also has 2 PS of Sweden Bridles I am selling since they are $$$. I can always get another bridle.
@theresak yes thats what it is. He was actually doing much better and laying down about 3 nights a week. I have been working on this since I got him. But I wondered if something in his neck, also effected this.
It definitely could be pain in his neck causing him to not want to sleep lying down. It’s something I haven’t totally ruled out as part of the cause for my horse, but I think a lot of his issue is due to changes in the herd (lost the herd leader), stall neighbor leaving, and a 7 month stall rest that all happened together.
Also, do vets no longer use DMSO infusions for neuro/spinal issues? I would think this horse’s symptoms would be a potential case for DMSO treatment. I’m not 100% sure, but I think it has less risk of laminitis than steroids if that is a concern for the particular horse.
1 Like
I would not do chiro after a fall without doing xrays first. However, if you have a vet that does acupuncture, that could help with the muscle pain management right now.
As for blocking, yes, you can sometimes get improvement blocking the leg. IME, either there is also something going on in the limb (like arthritis) or the neck creates altered movement either uncontrollable “lameness” or a bracing/compensating pattern that can cause some uneven wear and tear.
So, with client’s horse that I have mentioned, his neck stuff based on images was not new, and at least one site to my eye looked like a congenital defect. But I think he had been compensating for it for years until it got to be too much from a pain/comfort perspective and also affecting him neurologically. He had some arthritis elsewhere, history of needing some joint support, etc. Also kind of clumsy. Clumsy started turning into eyebrow raising stumbles and forgetting to move the legs in the appropriate order such as when backing up. Initially looked kind of like hocks (routine thing). Injections very short lived. Then seemed to block to a fetlock where there was a known issue. But injecting that did nothing. Then seemed like high up, stifle and/or SI. Identified things in both places. Might have improved some blocking the stifle but not as much improvement as had been from blocking the fetlock. Injecting all of that twice also did nothing. During this time, front feet also became bilaterally sore and horse would block to the feet (but was horse just unloading the hind end and/or hitting the ground too hard hence the tripping? probably).
After much chasing body parts (which happened even after imaging the neck and finding issues from C4-T1, making me really question the particular vet’s judgment especially since I was given the job of exercising the horse), I suggested to client (who was in the process of moving) that horse go to the big equine hospital near his new home for a second opinion, at which time neck was concluded to be the primary issue and retirement was recommended.
1 Like
I too was wondering about the DMSO esp if you suspect there may be a recent fall.
I would hold off on Chiro with suspected neck issues. A friend found out that her horse did indeed have neck issues after a chiro adjusted him, he was Euthed within 24hrs.
Obviously this was an extreme outcome, but very distressing for her. By the time it was found then, his pain was beyond manageable. Horrible situation.
1 Like
My OTTB did something similar a couple of years ago. He had obviously been in a fight with his tape fence and had a very fat knee. He was also ataxic in his hind end. It wasn’t super obvious in walk (I could see it but equally experienced horse people could not) but he struggled to turn as he couldn’t step correctly around with his hind end. He couldn’t trot properly and failed the tail phll His neck had normal range of motion and his front end appeared to be unaffected. He was also very quiet although TPR was normal. The vet suspected a compressed nerve suspecting he had flipped himself.
He was given IV DMSO and bute for several days and was almost normal within a week. I turned him out for a couple of months anyway. He hasn’t had an issue since aside from being a prick to deal with which is unfortunately normal for him…
My OTTB did something similar a couple of years ago. He had obviously been in a fight with his tape fence and had a very fat knee. He was also ataxic in his hind end. It wasn’t super obvious in walk (I could see it but equally experienced horse people could not) but he struggled to turn as he couldn’t step correctly around with his hind end. He couldn’t trot properly and failed the tail phll His neck had normal range of motion and his front end appeared to be unaffected. He was also very quiet although TPR was normal. The vet suspected a compressed nerve suspecting he had flipped himself.
He was given IV DMSO and bute for several days and was almost normal within a week. I turned him out for a couple of months anyway. He hasn’t had an issue since aside from being a prick to deal with which is unfortunately normal for him…
I’m following this with interest, because I feel different vets have different opinions on CA/wobblers/neck related neuro.
I had a horse that had both neck X-rays & bonescan done and what was seen in the neck remained inconclusive & questionable, he was slightly neurological in the hind and also had on & off hindlimb lameness that did not block out in the leg.
It was explained to me that a wobbler you will know early on in life and it causes neuro issues, propioceptive deficits in the hindlimbs, off-movement, toe drag, weakness etc. but not necessarily a pain lameness.
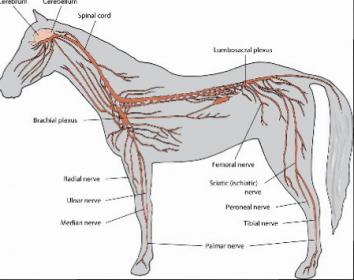
Cervical arthritis can definitely cause lameness and pain but such will show up in the front limbs, not in the hindlimbs. If you have a hindlimb lameness that is due to spinal issues, this will be from end thoracic/lumbar to scacral spinal arthritis or nerve compression, more specifically femoral and sciatic nerve.
Wobblers would be a spinal cord damage originating deeper in the cervical spinal cord, which thereby causes hindlimb propioceptive problems, whereas cervical arthritis or arthritis further down the spine will affect the outer nerves of the cord thereby can give front limb lameness in case of cervical arthritis but not hindlimb lameness, latter would be due to thoracic/lumbar spine arthritis.
I included a picture of the where the nerves originate and all cervical nerves run down into the front limbs, lumbar/sciatic nerves run down in the hindlimbs with thereby corresponding lamenesses?
I’d be curious what you all think of this, it’s hard to discuss when vets have different opinions.
wow this gives me some hope! Thank you everyone for all your insight. It is helping me stay positive.
The vet never recommended DMSO. Just Dex. Yesterday he looked good. He came in at noon though because it was 40 degrees and they were all drenched in sweat. He was in until this morning, and leaving his stall he seemed more wobbly than the last few days and toe dragging worse. I was wondering if that might be because of him not moving around as much the last 16 hrs.
Otherwise, his spirits are really good. He has the same great appetite. Before this he never showed any signs of issues. He has been very sound, and a joy to ride and train since the day I got him. He did race until 9, 77 starts.
Keep in mind Wobblers is a catch-all term. It in itself is not a diagnosis.
Re: the bold - I am not certain that is true. It has not been true in my experience. Perhaps the two are related, in that horses with congenital neck defects might tend to also have spinal defects (thoracic/lumbar) – but cervical arthritis can and does cause proprioception issues behind in my unfortunate experience with CA cases.
One of the most common symptoms of cervical arthritis in my experience is listing to the side and general hind end weakness.
There are many prominent stallions that were “wobblers” - or, specifcally, had compression/narrowing of the spinal cord originating in the neck – these stallions had well-documented early lives and did not demonstrate neurologic or proprioceptive issues until they were advanced in years; if anything, I’m seeing more of it in older horses than younger horses.
Good point! Likely there was enough space in the spinal cord when they were younger and the compression got worse with age or inflammation set in etc.
Thank you beowulf.
Did you horse with CA have a hindlimb lameness as well as loss of propioception? With hindlimb lameness I mean, where you can tell it’s hurting somewhere?
This particular vet was of the opinion lameness from CA, would show up in the front limbs only.
Hard to find good literature and evidence on how far down CA can affect a horse and cause lameness, I researched this a fair bit, but didn’t get the answers I was looking for, it’s interesting to hear from people’s experiences.
Hogwash. Maybe that’s the old thinking, but it’s been well documented that c spine arthritis can cause hind limb lameness.
If you have films and a bone scan that your local vets are unsure how to interpret, package it up and send to Martinelli in California.
3 Likes
CA can cause front limb lameness if the nerve roots that are affected are nerve roots to the front legs. CA can cause hind limb lameness that has no other explanation. CA can cause no lameness. And this can change over time. You can have shifting lameness or no lameness that turns into lameness depending on disease progression, status of inflammation, compensatory patterns, reduced ability to compensate (such as in the sleep deprived horse, older horse, etc.).
“Wobblers” is a catch-all term but more commonly Wobblers syndrome refers to spinal cord compression resulting from developmental abnormalities in a young horse. A true Wobblers case is likely to be under 4 years old. However, it’s also used to refer to cases of spinal cord compression generally, which can occur at any age and due to a number of factors such as unstable joints in the neck, trauma causing sudden onset compression, and is also sometimes used to describe CA or other degenerative disease that has progressed to the point of causing significant nerve issues, spinal column narrowing, and compression (in the latter case, the term is probably thrown around once the horse is 3/5 on the neuro scale, meaning has significant neurological deficits).
We know from human research that images of the neck (xray, MRI, etc.) do not necessarily correlate to pain (nerve pain or otherwise). There have been studies where radiologists were given these images and told to estimate the patient’s pain on a scale. The radiologists’ determination based on the severity of issues on the images basically had no correlation to what the patient was actually experiencing.
So, when it comes to non-Wobblers cases (meaning anything less than obvious spinal compression), it’s kind of a crapshoot in determining the level of pain, what kind of pain, and whether the pain is related to any location of nerve issues (if there are any apparent nerve issues such as proprioceptive lameness, ataxia). Sometimes you can measure how well specific nerve roots are firing with EMG type studies. But a proprioceptive deficit does not necessarily mean there’s pain in the affected limb, although it can contribute to gait imbalances that eventually strain ligaments, tendons, joints, cause more concussion in the foot, pulled shoes, etc.
IME, ataxia such as OP’s horse is experiencing from sudden trauma needs to be evaluated for acute injury first to the back, pelvis, and neck (and may resolve when the actue inflammation is resolved) but then as beowulf says, the fall could have been caused by what had been mild proprioceptive deficits already occurring, and investigating that is important if we want to try to prevent another similar trauma (or even worse, if something bad happens jumping XC).
3 Likes
Thank you Simkie, I didn’t dare to disagree with him at that time and had nothing to counter his thought process, but yes with the latest advances in vet med, he probably was still going by old school thinking.
IPEsq, great post, thank you, you are pretty much summing it up. Crapshoot indeed.
I agree the original poster should make sure there’s no obvious hindend trauma and then move on to what may have been there all along and missed.