
So sorry you’re not doing well. A few additional opinions at this point would be an excellent idea. Definitely don’t just go back into the joint with the same surgeon.
1 Like
The surgeon seemed to imply that I was saying he did a bad job. I was thinking “no dude, I know what I do is hard on the hips”.
Did you have to find another surgeon? Did you have FAI or just the tears?
Thanks, I don’t think he actually did anything wrong. I just think we equestrians put stresses on those joints that most people don’t. And I know I’m built funny. My hips have always turned inward, from birth.
Plus I fell off hard around 6 months out from surgery…hit the right hip but couldn’t have been good for it  Horse spun and I failed to.
Horse spun and I failed to.
It’s not about assigning blame or saying what he did was “wrong.” This is a very new field, and knowledge/experience isn’t at all evenly dispersed across the surgeon population. It’s often finding just the right person to identify the issue & correct it.
Impingement doesn’t regrow in a year. Hips “turning inward” suggests a version abnormality. Did you have a pre op 3D CT to evaluate acetabular undercoverage, acetabular version and femoral version? All of these things can impact success.
Your outcome matters a whole lot more to you than to him. Go get a few more opinions, and see what other experts think.
1 Like
I had FAI and tears. The first one took years to diagnose, Simkie is the one that actually figured it out thank God. The right hip tore while rehabbing from the first surgery on the left. The right tore again later when I twisted a certain way while mowing the lawn. The repair to the right one looked perfect when they were fixing the second one so the operation was a success. They have to be conservative when taking the impingement down because if they take too much it will make it easier to dislocate your hip.
2 Likes
I had a pre-op MRI with dye to show the tears. The impingement was obvious in both the MRI and the X-rays - huge bumps on the thigh bone initially and on the socket. It wasn’t just a long socket, it had a lump in it as well. I don’t know how well he evaluated the coverage and version. Would that be in my report?
The camera was in there for the operation and final pictures, so I saw the shaving area on both the thigh bone and the hip side - and we had X-rays afterward that showed smooth spherical bone. There is no longer smooth bone, the bump is back, and it’s not the same size, but it’s definitely there.
Originally, the tears were bad (one was completely shredded) but I didn’t feel them unless I sat in my dressage saddle. I didn’t discover either for years because I was riding hunters with short stirrups and didn’t need to open my hips. I just thought I was inflexible and kept shortening my stirrups LOL - but I did notice that I appeared more and more to be in a chair seat, which wasn’t normal. I just thought I needed to stretch.
But I could run and walk without pain. Then I ended up with severe pain in my feet which I think has to be connected. They called that an abnormal plantar fasciitis, but that went away after my surgeries which led me to believe that I was now “tracking straight” post surgery.
I’m no longer tracking straight walking, I have the mildly pigeon-toed on the right leg and definitely pigeon-toed on the left leg appearance again. It’s a distinctive gait (again, I always just thought I walked weird). When I try to ride, once again my leg gets “stuck”. It’s not the “muscles won’t go” feeling, it’s the “leg cannot move anymore feeling”. The times it hurts the most are after I’ve been on my feet for awhile and I just…step funny. I take a step backward or I twist to clean a stall and yowza.
I have an appointment with a second doctor in December. The whole process is frustrating.
Version is orientation in space. The acetabulum sits in the pelvis and can “point” very forward (excessive anteversion, abnormal), forward (anteversion, normal), or rearward (retroversion, abnormal.) The neck of the femur has similar possibilities.
These things need CT to evaluate, not MRI. Femoral version relates to the femoral condyle in the knee, so imaging needs to go knees to pelvis.
Here’s a graphic, this really helps illustrate:
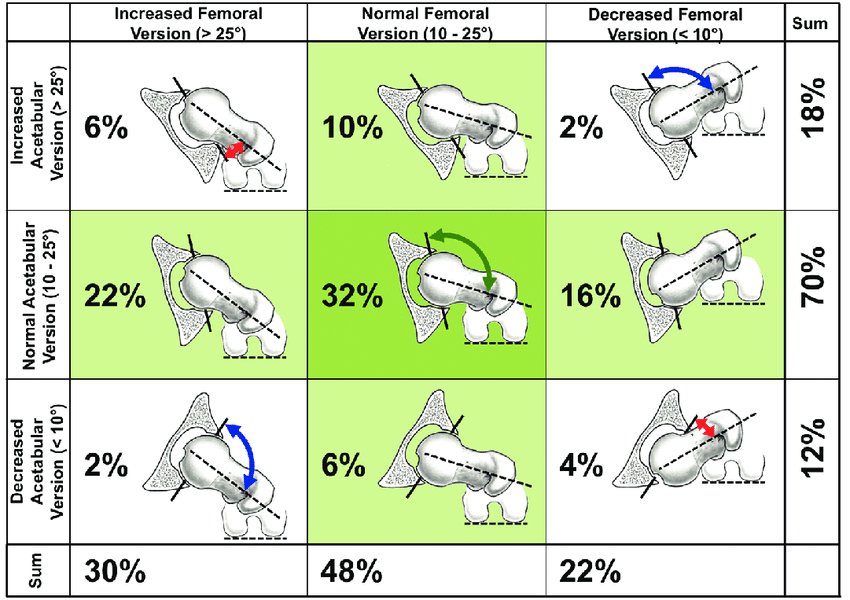
Hip version issues can be compounded by knee and ankle version issues.
Bringing the knee inward toward midline within the stride is stabilizing an unstable hip, which might be what you’re doing and seeing as “pigeon toed.”
If the hip is unstable, taking more off the acetabular rim will only destabilize you more. Instability causes extra articular pain in the muscles surrounding the joint, because they’re working overtime to keep you together. Instability also causes the labrum to tear again.
Degree of instability can be evaluated with dynamic ultrasound, but it’s a novel imaging technique and very few offer it at this time.
Assessing failure following hip arthroscopy is often murky. Arthroscopists often ignore or disregard greater structural issues in the hip. There’s very little consensus in the field, it’s a lot of guys doing their own thing. Lots of people go through an unsuccessful scope, or a few of them, before getting to the right surgeon to diagnose a structure issue.
(I’m intimately familiar with this–my labral reconstruction was a miserable failure. Imaging was called normal for YEARS. When I finally got a diagnosis, it was VERY OBVIOUS to that surgeon, and he made that diagnosis from the CT that had been called normal by several other “top” surgeons. And that’s just not uncommon, unfortunately.)
That’s awesome you’ve lined up someone else to see. I’d really encourage you to get a few additional opinions, from the absolute best surgeons you can find. Failure cases are complex, and every time you go into that joint and through the capsule, you’re adding a degree of instability and trauma. I would be happy to recommend a few, if you’d care to share where abouts you are in the country.
3 Likes
Thank you - Chloisy is one you recommended upthread and that’s who I’m going to see in December.
Based on the graphic and a little google-fu, it appears that I have femoral anteversion. I was a W sitter as a child, and still struggle to sit butterflied. Maybe there’s hope that another round of physical therapy can help me.
Ah that’s fantastic!! Ask him about a CT. I hope he’s got some solid answers for you!