Did they explain why it’s a no?
Eta im not arguing it is, I’m curious to understand their reasoning why. That would help us all towards better understanding

Did they explain why it’s a no?
Eta im not arguing it is, I’m curious to understand their reasoning why. That would help us all towards better understanding
Congrats to you for digging til you got someone who could listen and explore
I went through a similar, but much shorter journey when my horse started down the DSLD road, so I get it.
It’s not good news per se, but damn it’s nice to be on the right freaking road!
The Texas A&M vet did not explain her rationale for why she didn’t think he had either of those 2 conditions. Likely the same reason why she refused to do any further investigating and also telling me to stop looking for a reason why he isn’t improving.
The third vet did not think he has DSLD because he could see where the sources of pain were and he confirmed that by imaging. He also doesn’t think it’s DSLD because the PSD didn’t just show up out of nowhere and he disagreed that he has straight hocks. The PSD was a result of a right SI injury and when he stood camped under trying to relieve pain in his SI he strained his suspensory.
Thanks, sounds like you found excellent care finally.
I can finally come update now that I have the picture of his SI. His new vet is incredibly busy and when all his images came over the most important ones were missing. 
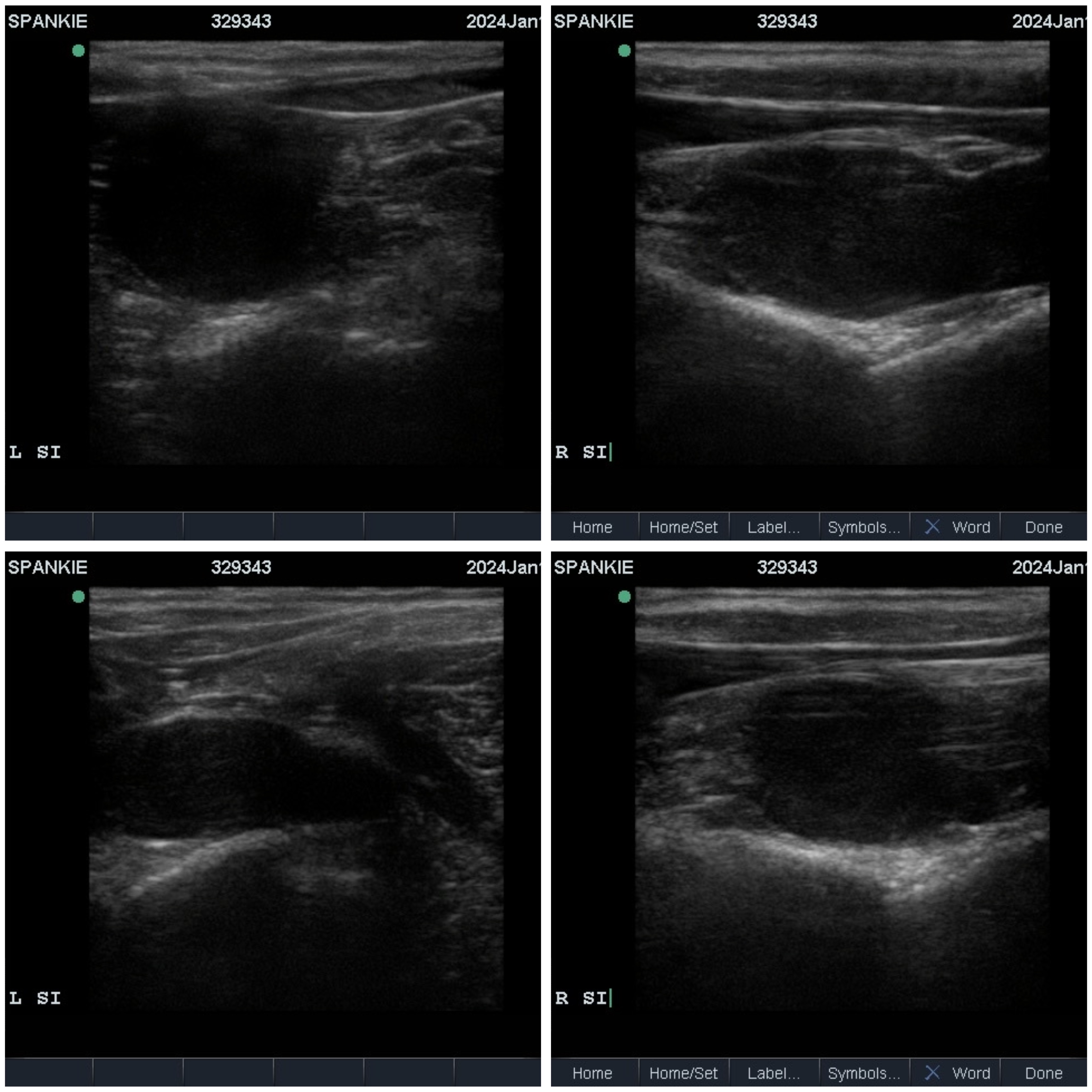
Without further ado here is the right SI compared to the left and the official diagnosis is ligament desmitis of the right SI. Vet said this was likely a pasture injury from when he was a foal and that he would have been significantly lame with this injury. He was turned out on large acreage so I think it was just honestly missed and he has lived like this forever.
I did give him about another 6 weeks off after he had his SI treated. We did some hand walking but more rest than anything. I just started his under saddle walking hacks for 10 minutes. He is so much more naturally forward and willing to march along with his ears pricked. I don’t have to use my crop to encourage him to simply walk. He has offered a half hearted trot and it doesn’t feel like he’s offering it out of freshness or silliness, he honestly feels workman like. He has this whole new range of motion over his back and in his hind end, so much so to the point that his hind shoes are interfering with his front shoes and he clicks his shoes which is new. He also has so much more support in the angles in his hind end. He has actual heels in his hind feet and the angles aren’t collapsed like they had been. We go back on march 1st to rescan his suspensory and then we will go from there and I’ll include updates.
I’m going to copy what was in his vet report with the new vet.
Neck Palpation: Focal pain response with deep palpation of the lower cervical spine region at the level of C6-7 bilaterally. Mild, focal muscle atrophy noted in the right caudal cervical spine musculature at the level of C6-7. Palpation of the mid and cranial cervical spine elicits no response. Cranial nerve reflexes are intact bilaterally, and cervical range of motion is symmetric bilaterally, but stiff/slightly limited with lateral flexion of the lower cervical spine (reaches heart- girth bilaterally, but r e s i s t s to flank)
Back Palpation: No pain response is noted on deep palpation of dorsal spinous processes or epaxial musculature. Induced dorsiflexion, vetroflexion, and lateral flexion at the thoracolumbar junction is symmetric and free of notable pain response. Beginning at the level of the thoracolumbar junction, subtle atrophy is noted ni the right lumbar epaxial musculature, extending to the level of the tuber sacrale. The right gluteal region is also subtly atrophied in comparison to the left side
LF Palpation: Mild medial to lateral imbalance of the left front foot (low medially). No swelling, heat or sensitivity noted in the distal limb, and ful range of motion is noted ni the lower limb, free of pain response. Negative hooftester exam. Palpation of the scapular and cubital regions are unremarkable.
RF Palpation: No swelling, heat or sensitivity noted ni the distal limb, and ful range of motion is noted in the lower limb, free of pain response. Negative hooftester exam. Palpation of the scapular and cubital regions are unremarkable. Mild positive hooftester over central frog.
LH Palpation: Mild medial femorotibial effusion palpable. The plantar metatarsus is clipped from prior ultrasound exam. No tarsal effusion noted, No pain, heat, sensitivity or swelling is noted ni the lower limb. External/internal rotation, abduction, and adduction of the limb is well tolerated by the patient and is unremarkable. Deep palpation of the gluteal regions and pelvis elicit no response. Negative hooftester exam
RH Palpation: Mild atrophy noted to the right gluteal region, medial thigh region (semimembranosus/semitendinosus). No pain response elicited with deep palpation of pelvic/sacral regions, external/internal rotation of the limb is well tolerated Abduction of the upper limb meets moderate to marked resistance by the patient, especially asymmetric to the left. No heat, swelling, or effusion noted in the lower limb. The plantar metatarsus is clipped from prior ultrasound. Moderate reaction noted by the patient with deep palpation of the proximal suspensory region. Range of motion of the distal limb is unremarkable. Palpation of the suspensory branches yields no pain response, and mild subjective asymmetry between lateral and medial branches. When asked to stand square, the horse consistently externally rotates the limb, placing the limb cranial to the left at rest. Mild positive hooftester over frog
Additional Lameness Findings: Lameness examination was attempted on the lunge line on level soft footing, and gaits above a trot were not obtained in an effort to reduce the chance of exacerbation of the historic suspensory desmopathy. On the lunge to the left at a trot, a mild consistent right hind limb lameness was noted and the patient consistently drifted into the circle, leaning inward with the pelvic region. Trotting to the right was resisted by the patient with rearing and reluctance to move forward.
Radiographs:
Cervical Spine: Moderate enlargement of the articular process joints at the level of C6-C7 si noted with mild ot moderate osseous irregularity at the caudal joint margin of the right articular process joint. Smooth blunting of the right ventral lamina is noted compared to the left along the caudal margin, but the left and right ventral laminae of C6 are present bilaterally. Articular process joints of the cranial and mid cervical spine are unremarkable as is the poll and basilar skull region
Thoracolumbar Spine: An ovoid, linear region of dystrophic soft tissue mineralization is noted in the area of the nuchal ligament/supraspinous ligament along the Withers. No overriding dorsal spinous processes are visible, and thoracic/cranial lumbar spine regions appear unremarkable
Ultrasound:
Thoracolumbar Spine:
Articular process joints of the thoracolumbar region appear unremarkable and free of periarticular osteophytes or visible new bone production. The multifidus muscle throughout the thoracolumbar region appears symmetric in terms of size and echotexture bilaterally. No obvious areas of atrophy are appreciated
Transrectal Ultrasound: The right iliopsoas muscle is palpably smaller than the left throughout the palpable extent of the muscle, subjectively. No obvious pain response is elicited with transrectal palpation of the muscle, however sedation was performed prior to rectal exam for safety. Transrectal ultrasound of the L6- S1 disc space as well as the L5-L6 disc space was performed and found to be unremarkable. Ultrasound examination of the intertransverse joints was unremarkable bilaterally, along with transrectal examination of the L6-S1 and S1- S2 neural foraminae. Ultrasound examination of the ventral aspect of the sacroiliac joints, transrectally, revealed an asymmetric thickening of the ventral sacroiliac ligaments of the right side when compared ot the left, with a motled heterogenous echotexture.
Diagnosis: Resolving Bilateral Proximal Suspensory Desmopathy Right Sacroiliac Pain/Chronic Desmopathy
Bilateral C6-7 Articular Process Joint Osteoarthropathy
Treatment Plan: Based on the clinical examination, combined with transrectal ultrasound findings, right sacroiliac pain along with a chronic desmopathy is suggested as an additional component of the lameness. The historic RH proximal suspensory desmopathy is still considered active, with prior localization of the lameness to the proximal
metatarsal region, prior ultrasound findings of suspensory desmopathy, and residual right hindlimb lameness. The source of the predominant right hind lameness today is thought to be associated with the proximal suspensory injury primarily, however diagnostic anesthesia was not repeated to confirm this, as ti had been recently performed at Texas A&M.
Blood was aseptically harvested and from the jugular vein and processed to obtain autologous platelet rich plasma. Under ultrasound guidance, after aseptic preparation of the site, each sacroiliac joint was injected from the cranial approach with platelet rich plasma. Using platelet poor plasma, the origin of each iliopsoas muscle was injected under ultrasound guidance between the transverse processes of the L5 and L6 vertebrae, bilaterally.
Under ultrasound guidance, the left and right C6-7 articular process joints were injected with amikacin and 6 mg of betamethasone.
Medication: Phenylbutazone: We recommend administration of 1gram orally twice daily for 3-5 days after injection Controlled exercise plan:
Week :1 We recommend 1week of rest post-injection, consisting of stall and or small paddock rest. During this time we recommend baited stretches (“carrot stretches”) to promote mobility and range of motion of the cervical, thoracic, and lumbar spinal regions. Stretches should be performed to the point of the shoulder, then the carpus, then the foot on both sides, then progressing to the heart girth, and then to the hock on both sides. Stretching should continue for total of 3 to 5 minutes daily, and should continue throughout rehabilitation.
Week 2-3: We recommend beginning under saddle exercise with 15 minutes walking daily.
Week 4-8: Please begin with a 10-minute walk under saddle on level footing, followed by 3minutes trotting ni straight lines, finishing with a 10-minute walk. Please add 2 minutes trotting per week, continuing in straight lines
until week .5 At this time he may begin ot trot ni large, arena-sized circles. When trotting, the goal si for collection of the head and neck, and extension of the hind limbs (long trotting). The goal ni this form of conditioning is an increase in core body strength and gluteal musculature. This may be also achieved with commercially available
lungeing systems such as the Pessoa system.
Acupuncture, massage, and PEMF therapy are ancillary treatments that may be considered during rehab, and may improve the existing muscle atrophy.
Hind end engagement exercises are also useful, such walking over ground poles and cavaletti exercises. To begin, these exercises should be done at a walk, but may increase ni speed/intensity as rehab progresses.
Please monitor for any increase in lameness, swelling, heat or drainage from the injection sites. During controlled exercise, please monitor for any worsening of lameness or exacerbation of gait deficit or stance at rest. fI any of these are noted please reduce exercise and contact Brazos Valley Equine Hospital as soon as possible.
Please schedule recheck lameness exam in 6 to 8 weeks.
(I copied this from a pdf on my phone and I think it’s picking up spelling errors that aren’t really there sorry about that!)
export_1708915562611
Looking great. So glad you finally nailed down what is going on. The recovery protocol looks very manageable.
I had a gelding with an SI tear, it was also very difficult to diagnose at the time and I remember a lot of vets chalking it up to behavioral until I went to a lameness specialist. It was a long layup. Injections to the SI site made a night and day difference for him.
After treatment you acquired a cat! I love that slinky free walk. I am glad you got some answers.
Wow, he looks so much better! So glad you kept searching for answers for him! Hope he continues to improve.
Thank you all so much!
Wow, that’s really impressive!
I had NO idea that walk was in there. He was winning dressage moving like the top video. He’s going to be incredible when he’s recovered. I’m so excited to see how his other gaits have improved as well as his jump. His whole hind end is so much more improved, from his hooves to the angles. He is supported. He’s not compensating from pain. I feel like when he gains his strength and fitness this time it will stick and he will be able to maintain and I’m hoping that really affects his prognosis and his future. I’m so glad I have a vet now that understands us and I will know where to look if he starts to decline at all. 
Just got done with his 6 week rescan of his suspensories. The branch desmitis has resolved and the rest was deemed compensatory with one tiny little spot evident on the right medial proximal suspensory. I think he said it looks like a micro tear that healing and very tiny. One more month of increasing the duration of walk before we introduce 1 minute trot intervals. Will rescan in 8 weeks. When he gets to 10 minutes of trot it should be time to allow his regular turn out again. 
He said the progress made with his SI and pelvis has improved more than he was expecting and I showed him the videos of his walk side by side and what a huge difference it is. He has full range of motion in his pelvis and was unreactive to deep neck palpation. Yay!
That’s really great!
Great news! 🥹
Continuing the discussion from Proximal Suspensory Desmitis:
Hi everyone. I’ve been reading this thread and would love any advice that could be given in regards to my current situation. I have a 4 year old OTTB that I got about a year and a half ago. About 3 months ago at the beginning of December, he came up lame on the LH. With the effusion in the tendon sheath, my local vet wanted to be cautious and had me put him on stall rest for a month. He was then diagnosed mid January with prox suspensory desmitis after hauling him to a vet 4 hrs away that has many years of experience with lamenesses and surgeries. The ultrasound showed no tears or lesions, just that the suspensory measured .14 cm bigger than the RH. We injected with steroids and shockwaved that same day and I was instructed to small paddock turn out for another month and then re-evaluate again. I kept him in a very small paddock (maybe 30x50 ft) and had to keep him sedated pretty much every day.  After a month and a half, we were able to reassess and he was still significantly lame and only became better after blocking.
After a month and a half, we were able to reassess and he was still significantly lame and only became better after blocking.
All that said, I’m now highly considering surgery because this poor guy is so young and had endless potential. He was bought in the hopes of being my next upper level event horse, but the injury came before he even made it to a first event. I have taken things EXTREMELY slow due to the fact that he wasn’t even 3 when I purchased him. Due to that and life circumstances, I’d only just really gotten him into a consistent program maybe 6 months prior to the injury, and he was only being ridden 3-4 days a week.
I’ve done tons of research and all the info I read says there’s a 70% chance after surgery that he will go back to the level of work he was in before the injury, and that’s also what my vet told me. But the horse was hardly doing much of anything before this, so I’m wondering realistically if he’ll be able to event or if I should accept the fact that he might just have to be a dressage horse.
I’m dying to know if anyone out there has had a similar case with a young horse that had the surgery and was then able to go on to have a successful and limitless career? Like I said, my horse was maybe jumping a few times a week, and only prob 2-2’3. We had probably really only been in a consistent work routine for 6 months prior to the injury. He is pretty straight behind, so I’m guessing his conformation and breed played a part in the injury, but it’s just mind blowing to me that this level of work made him lame but he was totally sound in race training. I even have a video of him at the OBS 2 year old sale galloping a furlong flat out in under 10 seconds. I’m terrified the injury was caused due to the fact that I don’t have an arena yet at my place and the terrain is inconsistent. But I’ve always been great about hauling off property to use an arena if the footing isn’t ideal bc I don’t want to tear up my field.
Anyway, hoping I can get some more knowledge from this group and would appreciate hearing any experiences you’ve had! Thanks you!
Realistically dressage is pretty demanding on suspensories.
Being “just a dressage horse” would be a very good outcome…
The N/F surgery would potentially help him, how it would be for you is another story.Would you be prepared to pay for the surgery, do the box rest or pay for a rehab fascility,do the rehab and maybe end up with a 4yo retiree anyway?
You will certainly be left with a suspensory issue that will need monitoring always, careful warmups, good working surfaces (late night sleepless worrying lol)
The surgery is JUST the beginning…you will learn a lot and deepen your understanding of horses though, so that’s something good!
One of the anxiety causing problems for me was that nobody can tell you if or for how long or how well it’s going to work .
If I personally had 4yo OTTB with this issue and could retire him,I would.If the surgery was his only chance to stay alive i’d do it but I would really prefer never to rehab a suspensory again .
If you do really adore him and want to do everything you can for him you need to be aware that it’s a big big job that may not yield the results you’re hoping for and be OK with that going in.
Best of luck to you both.
Personally, I’m not a huge proponent of the neurectomy part of any surgery TBH, but I have done the fasciotomy (and admittedly my horse wasn’t a candidate for the neurectomy so I didn’t have to even consider it). If the horse doesn’t have a tear/lesion and it sounds like its just swelling, you can do just the fasciotomy, which is what I have done. But I’d also give a Class IV laser a go first. It’s been the only thing that has worked to get the swelling out post op both times so if the swelling of the ligament isn’t awful it may resolve it w/o surgery.
Agree with the above poster that dressage is very hard on horses’ hind ends. Dressage horses actually have their fair share of suspensory injuries as well due to the loading needed for the engagement at 3rd and up. The difference between dressage and eventing is the surface/footing is better maintained and predictable whereas XC who knows what you might encounter. I’ve balanced those and decided (and discussed with my vet team and farrier) that if they think my guy can do 3rd level dressage, he can bop around BN/Novice. But I’m fortunately the venues near me are basically golf courses.
Thank you for the input! I guess I should have specified it as “just a lower level dressage horse.” I understand how much strain higher level dressage puts on the hind end with the engagement and collection required. I have previous experience taking care of and handling rehabbed racehorses, so I feel prepared to take on the rehab that is required post surgery. I’ve definitely come to terms with the fact that even after the surgery he may not be sound, but I feel I owe it to him to try since he’s still significantly lame after 3 months of restricted turnout to a small paddock. I would love if his body would let him reach his fully potential, but I want more for him to just have a decent quality of life.
Thank you for the advice and info about your journey with the surgery! I will definitely look into the laser treatment!